Autoimmune thyroid diseases (AITDs) are common disorders marked by the presence of thyroid autoantibodies. This review summarizes their immunological roles, clinical relevance, and diagnostic value based on studies published up to January 2026. The main antibodies—anti-TPO, anti-Tg, and TSH receptor antibodies (TRAb) —serve different functions. TRAb play a direct pathogenic role, especially in Graves’ disease, while anti-TPO and anti-Tg are primarily markers associated with autoimmune thyroid destruction, such as in Hashimoto’s thyroiditis. Clinically, TRAb are important for diagnosis and monitoring of Graves’ disease, whereas anti-TPO and anti-Tg help identify autoimmune origin and assess the risk of hypothyroidism. However, their diagnostic accuracy is limited by their presence in some healthy individuals. Overall, thyroid autoantibodies remain essential tools in clinical practice, though careful interpretation is necessary. Future approaches combining immunology with computational methods may improve disease prediction and management.
| Published in | Science Discovery (Volume 14, Issue 2) |
| DOI | 10.11648/j.sd.20261402.12 |
| Page(s) | 24-34 |
| Creative Commons |
This is an Open Access article, distributed under the terms of the Creative Commons Attribution 4.0 International License (http://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution and reproduction in any medium or format, provided the original work is properly cited. |
| Copyright |
Copyright © The Author(s), 2026. Published by Science Publishing Group |
Thyroid, Autoantibodies, Autoimmune Thyroid Diseases, Hashimoto’s Thyroiditis, Graves’ Disease
TRAb type | Mechanism of action | Effect on thyroid hormone production | Clinical significance |
|---|---|---|---|
Stimulating (TSAb) | Binds TSH receptor, activates c Adenosine monophosphate (cAMP) signaling | ↑ T4 and T3 → hyperthyroidism | Primary driver of Graves’ hyperthyroidism; predicts relapse risk |
Blocking (TBAb) | Competes with TSH for receptor binding | ↓ T4 and T3 → hypothyroidism | Can cause hypothyroidism; relevant in postpartum thyroiditis |
Neutral | Binds receptor without functional effect | No significant change | Clinical role unclear; research ongoing |
Anti-TPO | Anti-Tg | TRAb | Likely Diagnosis |
|---|---|---|---|
+ | ± | — | Hashimoto’s thyroiditis |
+ | ± | + | Graves’ disease |
— | + | — | Seronegative Hashimoto’s |
+ | — | — | Euthyroid AITD |
— | — | + | Graves’ disease (early or isolated) |
± | ± | — | Postpartum thyroiditis |
Systemic autoimmune disease | Prevalence of Anti-TPO / Anti-Tg | Shared genetic susceptibility | Immunopathogenic mechanisms | Clinical implications | References |
|---|---|---|---|---|---|
SL | ↑↑ compared to general population, even in euthyroid patients | HLA-DR, HLA-DQ, CTLA-4, PTPN22, FOXP3 | Chronic B-cell hyperactivity, impaired apoptotic debris clearance, type I IFN signaling | Subclinical thyroid dysfunction may exacerbate fatigue, cognitive and metabolic symptoms | [37] |
T1D | ~30% may have anti-TPO / anti-Tg, often preceding clinical AITDs | HLA-DR, HLA-DQ | Autoreactive T lymphocyte-mediated beta cell and thyroid attack | Supports early thyroid monitoring; reflects polyautoimmunity | [38, 39] |
RA | Elevated vs. matched controls | HLA-DR, PTPN22 | Th1/Th17 polarization, epitope spreading | Associated with higher RA severity and extra-articular manifestations | [40] |
AITDs | Autoimmune Thyroid Diseases |
TPO | Thyroid Peroxidase |
Tg | Thyroglobulin |
TRAb | TSH Receptor Antibodies |
TSAb | Thyroid-Stimulating Antibodies |
TBAb | Thyroid-Blocking Antibodies |
TSH | Thyroid-Stimulating Hormone |
T3 | Triiodothyronine |
T4 | Thyroxine |
HLA | Human Leukocyte Antigen |
CTLA-4 | Cytotoxic T-lymphocyte-associated Protein 4 |
PTPN22 | Protein Tyrosine Phosphatase Non-receptor Type 22 |
FOXP3 | Forkhead Box P3 |
IL | Interleukin |
IFN-γ | Interferon Gamma |
TNF-α | Tumor Necrosis Factor Alpha |
RA | Rheumatoid Arthritis |
T1D | Type 1 Diabetes |
SL | Systemic Lupus |
DTC | Differentiated Thyroid Carcinoma |
ELISA | Enzyme-linked Immunosorbent Assay |
RIA | Radioimmunoassay |
CLIA | Chemiluminescent Immunoassay |
| [1] | Syrenicz A. Etiopathogenesis and diagnostics of autoimmune thyroid diseases. Thyroid Res. 2015 Jun 22; 8(Suppl 1): A26. |
| [2] | Yoo WS, Chung HK. Recent Advances in Autoimmune Thyroid Diseases. Endocrinol Metab (Seoul). 2016 Sep; 31(3): 379-385. |
| [3] | Flynn SD, Nishiyama RH, Bigos ST. Autoimmune thyroid disease: immunological, pathological, and clinical aspects. Crit Rev Clin Lab Sci. 1988; 26(1): 43-95. |
| [4] | Tomer Y, Huber A. The etiology of autoimmune thyroid disease: a story of genes and environment. J Autoimmun. 2009; 32(3-4): 231-239. |
| [5] | Weetman AP. Autoimmune thyroid disease. Autoimmunity. 2004; 37(4): 337-340. |
| [6] | Simmonds MJ, Gough SC. Genetic insights into disease mechanisms of autoimmunity. Br Med Bull. 2005; 71: 93-113. |
| [7] | Antonelli A, Ferrari SM, Corrado A et al. Autoimmune thyroid disorders. Autoimmun Rev. 2015; 14(2): 174-80. |
| [8] | Effraimidis G, Wiersinga WM. Mechanisms in endocrinology: autoimmune thyroid disease: old and new players. Eur J Endocrinol. 2014; 170(6): R241-52. |
| [9] | Rose NR. Prediction and prevention of autoimmune disease in the 21st century: a review and preview. Am J Epidemiol. 2016; 183(5): 403-6. |
| [10] | McLachlan SM, Rapoport B. Autoimmune response to the thyroid in humans: thyroid peroxidase—the common autoantigenic denominator. Int Rev Immunol. 2000; 19(6): 587-618. |
| [11] | Figueroa-Vega N, Alfonso-Pérez M, Benedicto I et al. Increased circulating pro-inflammatory cytokines and Th17 lymphocytes in Hashimoto’s thyroiditis. J Clin Endocrinol Metab. 2010; 95(2): 953-62. |
| [12] | Bottazzo GF, Pujol-Borrell R, Hanafusa T, Feldmann M. Role of aberrant HLA-DR expression and antigen presentation in induction of endocrine autoimmunity. Lancet. 1983; 2(8359): 1115-19. |
| [13] | Glick AB, Wodzinski A, Fu P, Levine AD, Wald DN. Impairment of regulatory T-cell function in autoimmune thyroid disease. Thyroid. 2013; 23(7): 871-78. |
| [14] | Stassi G, De Maria R. Autoimmune thyroid disease: new models of cell death in autoimmunity. Nat Rev Immunol. 2002; 2(3): 195-204. |
| [15] | McLachlan SM, Rapoport B. Thyrotropin-blocking antibodies and thyroid stimulating antibodies: potential mechanisms involved in the pendulum swinging from hypothyroidism to hyperthyroidism or vice versa. Thyroid. 2013; 23(1): 14-24. |
| [16] | Smith TJ, Hegedüs L. Graves’ disease. N Engl J Med. 2016; 375(16): 1552-65. |
| [17] | McLeod DS, Cooper DS. The incidence and prevalence of thyroid autoimmunity. Endocrine. 2012 Oct; 42(2): 252-65. |
| [18] | Rebuffat SA, Nguyen B, Robert B et al. Antithyroperoxidase antibody-dependent cytotoxicity in autoimmune thyroid disease. J Clin Endocrinol Metab. 2008 Mar; 93(3): 929-34. |
| [19] | McLachlan SM, Rapoport B. Breaking tolerance to thyroid antigens: changing concepts in thyroid autoimmunity. Endocr Rev. 2014; 35(1): 59-105. |
| [20] | Vanderpump MPJ, Tunbridge WMG, French JM et al. The incidence of thyroid disorders in the community: a twenty-year follow-up of the Whickham Survey. Clin Endocrinol (Oxf). 1995; 43(1): 55-68. |
| [21] | Huber G, Staub JJ, Meier C, et al. Prospective study of the spontaneous course of subclinical hypothyroidism: prognostic value of thyroid autoantibodies. J Clin Endocrinol Metab. 2002; 87(7): 3221-26. |
| [22] | Pearce SHS, Brabant G, Duntas LH et al. 2013 ETA guideline: management of subclinical hypothyroidism. Eur Thyroid J. 2013; 2(4): 215-28. |
| [23] | Chistiakov DA. Immunogenetics of Hashimoto's thyroiditis. J Autoimmune Dis. 2005 Mar 11; 2(1): 1. |
| [24] | Hutfless S, Matos P, Talor MV et al. Significance of Prediagnostic Thyroid Antibodies in Women with Autoimmune Thyroid Disease, The Journal of Clinical Endocrinology & Metabolism, 2011; 96: 9(1)S, E1466–71, |
| [25] | Vargas-Uricoechea H, Nogueira JP, Pinzón-Fernández MV, Schwarzstein D. The Usefulness of Thyroid Antibodies in the Diagnostic Approach to Autoimmune Thyroid Disease. Antibodies (Basel). 2023 Jul 22; 12(3): 48. |
| [26] | Spencer CA, Takeuchi M, Kazarosyan M, Wang CC, Guttler RB, Singer PA, Fatemi S, LoPresti JS, Nicoloff JT. Serum thyroglobulin autoantibodies: prevalence, influence on serum thyroglobulin measurement, and prognostic significance in patients with differentiated thyroid carcinoma. J Clin Endocrinol Metab. 1998 Apr; 83(4): 1121-7. |
| [27] | Dayan CM, Daniels GH. Chronic autoimmune thyroiditis. N Engl J Med. 1996 Jul 11; 335(2): 99-107. |
| [28] | Bahn RS, Burch HB, Cooper DS et al. Hyperthyroidism and other causes of thyrotoxicosis: Management guidelines of the American Thyroid Association and American Association of Clinical Endocrinologists. Thyroid. 2011 Jun 1;21(6):593-646. |
| [29] | Dwivedi SN, Kalaria T, Buch H. Thyroid autoantibodies. J Clin Pathol. 2023 Jan; 76(1): 19-28. |
| [30] | Barbesino G, Tomer Y. Clinical review: Clinical utility of TSH receptor antibodies. J Clin Endocrinol Metab. 2013 Jun; 98(6): 2247-55. |
| [31] | Stagnaro-Green A, Roman SH, Cobin RH et al. Detection of at-risk pregnancy by means of highly sensitive assays for thyroid autoantibodies. JAMA. 1990 Sep 19; 264(11): 1422-5. |
| [32] | Thangaratinam S, Tan A, Knox E, Kilby MD, Franklyn J, Coomarasamy A. Association between thyroid autoantibodies and miscarriage and preterm birth: meta-analysis of evidence. BMJ. 2011 May 9; 342: d2616. |
| [33] | Stagnaro-Green A. Postpartum thyroiditis. Best Pract Res Clin Endocrinol Metab. 2004 Jun; 18(2): 303-16. |
| [34] | Nicholson WK, Robinson KA, Smallridge RC et al. Prevalence of postpartum thyroid dysfunction: a quantitative review. Thyroid. 2006 Jun; 16(6): 573-82. |
| [35] | Moleti M., Sturniolo G., Di Mauro M., Russo M., Vermiglio F. Autoimmune thyroid diseases and pregnancy. Ann. Thyroid. 2018; 3: 18. |
| [36] | Zhernakova A, Withoff S, Wijmenga C. Clinical implications of shared genetics and pathogenesis in autoimmune diseases. Nat Rev Endocrinol. 2013 Nov; 9(11): 646-59. |
| [37] | Antonelli A, Fallahi P, Mosca M et al. Prevalence of thyroid dysfunctions in systemic lupus erythematosus. Metabolism. 2010 Jun; 59(6): 896-900. |
| [38] | Barker JM. Clinical review: Type 1 diabetes-associated autoimmunity: natural history, genetic associations, and screening. J Clin Endocrinol Metab. 2006 Apr; 91(4): 1210-7. |
| [39] | Kordonouri O, Klinghammer A, Lang EB, Grüters-Kieslich A, Grabert M, Holl RW. Thyroid autoimmunity in children and adolescents with type 1 diabetes: a multicenter survey. Diabetes Care. 2002 Aug; 25(8): 1346-50. |
| [40] | McCoy SS, Crowson CS, Gabriel SE and al. Hypothyroidism as a risk factor for development of cardiovascular disease in patients with rheumatoid arthritis. J Rheumatol. 2012 May; 39(5): 954-8. |
| [41] | Gupta AK, Kumar S. Utility of Antibodies in the Diagnoses of Thyroid Diseases: A Review Article. Cureus. 2022 Nov 8; 14(11): e31233. |
| [42] | Prentice LM, Phillips DI, Sarsero D et al. Geographical distribution of subclinical autoimmune thyroid disease in Britain: a study using highly sensitive direct assays for autoantibodies to thyroglobulin and thyroid peroxidase. Acta Endocrinol (Copenh). 1990 Nov; 123(5): 493-8. |
| [43] | González C, Hernando M, Cava F et al. Biological variability of thyroid autoantibodies (anti-TPO and anti-Tg) in clinically and biochemically stable patients with autoimmune thyroid disease. J Clin Lab Anal. 2002; 16(1): 37-9. |
| [44] | Michael L. LeFevre, on behalf of the U.S. Preventive Services Task Force. Screening for Thyroid Dysfunction: U.S. Preventive Services Task Force Recommendation Statement. Ann Intern Med. 2015; 162: 641-650. |
| [45] | Gao Y, Qiu L, Yu S, Cheng X. Thyroid stimulating receptor autoantibodies. Clin Chim Acta. 2024 Jun 1; 559: 119700. |
| [46] | Cho BY. Clinical applications of TSH receptor antibodies in thyroid diseases. J Korean Med Sci. 2002 Jun; 17(3): 293-301. |
| [47] | Manescu IB, Luca A, Hutanu A, Truta A, Dobreanu M. Anti-thyroid peroxidase (TPO) antibodies – Comparative analysis of two automatic methods, ECLIA and CMIA. Rev Romana Med Lab. 2024; 32(1): 33-40. |
| [48] | Wu JY, Zhang JY, Xia WQ et al. Predicting autoimmune thyroiditis in primary Sjogren’s syndrome patients using a random forest classifier: a retrospective study. Arthritis Res Ther. 2025; 27(1). |
| [49] | Luo T, Zhao X, Jiang X et al. Serum metabolomic analysis in patients with Hashimoto’s thyroiditis positive for TgAb or TPOAb: a preliminary study. Sci Rep. 2025; 15: 9945. |
| [50] | Rahmouni S, Dhifallah M, Mrad M et al. Prevalence and impact of thyroid dysfunction in patients with rheumatoid arthritis. Sci Rep. 2025; 15: 34491. |
| [51] | Rasoulizadeh Z, Eftekhar M, Ghadiri-Anari A et al. Prevalence of anti-thyroid peroxidase antibodies among women with polycystic ovary syndrome. Sci Rep. 2025; 15: 33563 |
| [52] | Bayrak Durmaz MS, Ozdel Ozturk B, Gorgulu Akin B et al. Autoimmune thyroid disease in inborn errors of immunity: a retrospective perspective. Orphanet J Rare Dis. 2025 Oct 23; 20(1): 536. |
| [53] | Liu J, Mao C, Mao X et al. T3 and T4 autoantibodies: emerging biomarkers for evaluating thyroid disorders. Front Endocrinol (Lausanne). 2025 Jun 12; 16: 1537222. |
APA Style
Zeroual, C., Mourabit, S., Moudatir, M., Echchilali, K., Barakat, L., et al. (2026). The Butterfly Code: A Mechanistic Review of Thyroid Antibodies. Science Discovery, 14(2), 24-34. https://doi.org/10.11648/j.sd.20261402.12
ACS Style
Zeroual, C.; Mourabit, S.; Moudatir, M.; Echchilali, K.; Barakat, L., et al. The Butterfly Code: A Mechanistic Review of Thyroid Antibodies. Sci. Discov. 2026, 14(2), 24-34. doi: 10.11648/j.sd.20261402.12
@article{10.11648/j.sd.20261402.12,
author = {Chaimaa Zeroual and Safaa Mourabit and Mina Moudatir and Khadija Echchilali and Leila Barakat and Hassan Elkabli},
title = {The Butterfly Code: A Mechanistic Review of Thyroid Antibodies},
journal = {Science Discovery},
volume = {14},
number = {2},
pages = {24-34},
doi = {10.11648/j.sd.20261402.12},
url = {https://doi.org/10.11648/j.sd.20261402.12},
eprint = {https://article.sciencepublishinggroup.com/pdf/10.11648.j.sd.20261402.12},
abstract = {Autoimmune thyroid diseases (AITDs) are common disorders marked by the presence of thyroid autoantibodies. This review summarizes their immunological roles, clinical relevance, and diagnostic value based on studies published up to January 2026. The main antibodies—anti-TPO, anti-Tg, and TSH receptor antibodies (TRAb) —serve different functions. TRAb play a direct pathogenic role, especially in Graves’ disease, while anti-TPO and anti-Tg are primarily markers associated with autoimmune thyroid destruction, such as in Hashimoto’s thyroiditis. Clinically, TRAb are important for diagnosis and monitoring of Graves’ disease, whereas anti-TPO and anti-Tg help identify autoimmune origin and assess the risk of hypothyroidism. However, their diagnostic accuracy is limited by their presence in some healthy individuals. Overall, thyroid autoantibodies remain essential tools in clinical practice, though careful interpretation is necessary. Future approaches combining immunology with computational methods may improve disease prediction and management.},
year = {2026}
}
TY - JOUR T1 - The Butterfly Code: A Mechanistic Review of Thyroid Antibodies AU - Chaimaa Zeroual AU - Safaa Mourabit AU - Mina Moudatir AU - Khadija Echchilali AU - Leila Barakat AU - Hassan Elkabli Y1 - 2026/04/30 PY - 2026 N1 - https://doi.org/10.11648/j.sd.20261402.12 DO - 10.11648/j.sd.20261402.12 T2 - Science Discovery JF - Science Discovery JO - Science Discovery SP - 24 EP - 34 PB - Science Publishing Group SN - 2331-0650 UR - https://doi.org/10.11648/j.sd.20261402.12 AB - Autoimmune thyroid diseases (AITDs) are common disorders marked by the presence of thyroid autoantibodies. This review summarizes their immunological roles, clinical relevance, and diagnostic value based on studies published up to January 2026. The main antibodies—anti-TPO, anti-Tg, and TSH receptor antibodies (TRAb) —serve different functions. TRAb play a direct pathogenic role, especially in Graves’ disease, while anti-TPO and anti-Tg are primarily markers associated with autoimmune thyroid destruction, such as in Hashimoto’s thyroiditis. Clinically, TRAb are important for diagnosis and monitoring of Graves’ disease, whereas anti-TPO and anti-Tg help identify autoimmune origin and assess the risk of hypothyroidism. However, their diagnostic accuracy is limited by their presence in some healthy individuals. Overall, thyroid autoantibodies remain essential tools in clinical practice, though careful interpretation is necessary. Future approaches combining immunology with computational methods may improve disease prediction and management. VL - 14 IS - 2 ER -
Department of Internal Medicine, Ibn Rochd University Hospital, Casablanca, Morocco
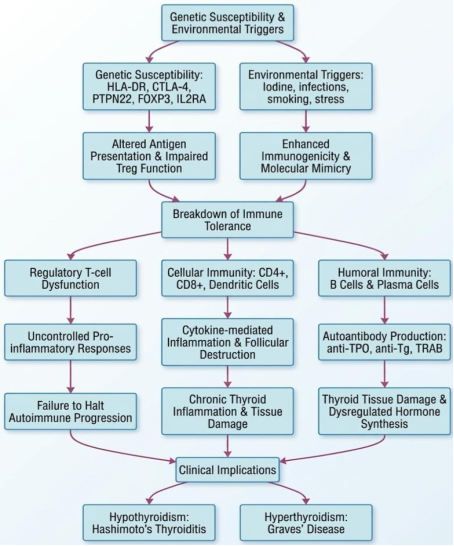
Figure 1. Pathogenetic mechanisms in autoimmune thyroid diseases. HLA-DR: Human Leukocyte Antigen – DR isotype, CTLA-4: Cytotoxic T-Lymphocyte Associated protein 4, PTPN22: Protein Tyrosine Phosphatase Non-receptor type 22, FOXP3: Forkhead box P3, IL2RA: Interleukin-2 Receptor Alpha chain, Treg: Regulatory T-cell, CD4+: Cluster of Differentiation 4 (Helper T-cells), CD8+: Cluster of Differentiation 8 (Cytotoxic T-cells), anti-TPO: Anti-Thyroid Peroxidase antibodies, anti-Tg: Anti-Thyroglobulin antibodies, TRAb: TSH (Thyroid-Stimulating Hormone) Receptor Antibodies
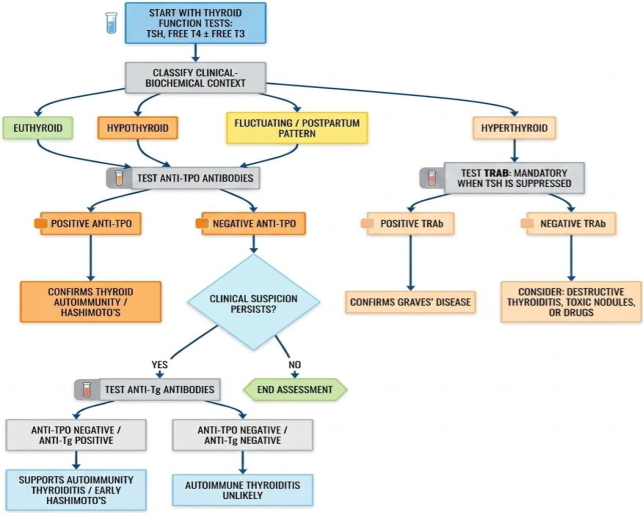
Figure 2. Antibody-based diagnostic algorithm in autoimmune thyroid diseases.
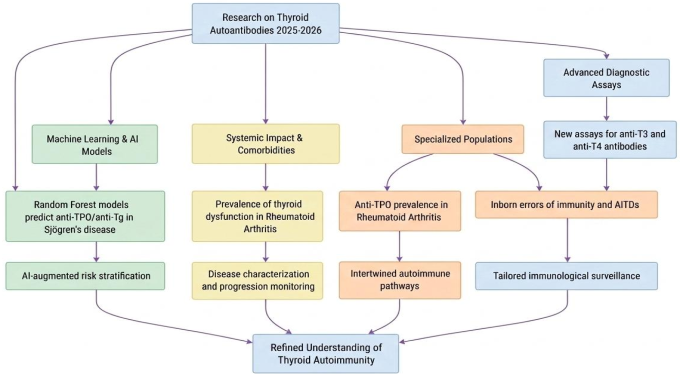
Figure 3. Research perspectives proposed for improving the understanding of thyroid autoimmunity.TSH: Thyroid-Stimulating Hormone, Free T4: Free Thyroxine, Free T3: Free Triiodothyronine, Anti-TPO: Anti-Thyroid Peroxidase Antibodies, Anti-Tg: Anti-Thyroglobulin Antibodies, TRAb: TSH Receptor Antibodies, AITDs: Autoimmune Thyroid Diseases, AI: Artificial Intelligence. Machine Learning: A subset of AI focused on building systems that learn from data. Random Forest: A specific machine learning algorithm that uses an ensemble of decision trees to make predictions.
Information

